How To Stay In Shape Even When You Have an Underactive Thyroid
I know just how hard life can be when you’re suffering with an underactive thyroid, but the reality is that if you’re prepared to put in a little hard work and dedication then there is nothing on this planet that is going to be able to prevent you from not only overcoming the symptoms of hypothyroidism but also getting into really incredible shape.
But the only way you’re going to be able to get long term results that matter is by first and foremost understanding and appreciating the fact that there are absolutely no shortcuts out there. The only way to get results is by making sure you are actually taking steps to implement a few core things.
The most important step of all is to ensure that the diet you’re on is super clean at all times. Diet is the one thing that you must work hard to perfect because without it you will never be able to overcome hypothyroidism and if you’re not able to do this then you’ll never be able to lose the weight that you want to lose! It’s as simple as that my friend.
The second part of the game is going be to make sure that you’re living a completely stress free life where you are enjoying every single moment that you have. If you’re stressed out then you’re body is going to be releasing stress hormones such as cortisol and this will ultimately result in you never being able to shed those excess pounds.
The third step is really simple and just involves you having to actually take the time to get out there and exercise as much and as often as you can. Exercise is the key to not only overcoming your underactive thyroid but also losing a lot of weight in a really short time frame. But know that you’ll very easily get results if you just put in the effort to create some sort of exercise routine that you can follow step by step.
The next step is going to be for you to ensure that you’re getting a good nights rest every single night. You have to give your body the chance to recuperate because if you don’t then you can totally forget ever getting over hypothyroidism for good! Rest is essential to give your body the chance to repair itself.
Overall I’d highly recommend that you enjoy every part of your journey. There’s no doubt that you are not going to eventually overcome your low thyroid and get into the best shape of your life, so why not actually take the time to enjoy the whole process. The better you get at doing this, the better your end results are going to be! It is as simple as that but it requires that you remain as strong and as faithful as possible. So waste no more time, just get out there and do whatever you can to take massive action.
High Capacity (Quality) Dentistry P2
So, I had to have a long, serious, hard discussion with myself as to what could work and couldn’t work in Ripley, Mississippi. So, at the time in the middle of this cosmetic craze, I’m charging $1200, $1300 for a crown, real fancy crown, and the guys down the street are charging $400. It’s hard to compete with that because around here it’s tough. People think a filling’s a filling, a crown’s a crown. It’s commoditized.
So, I thought I really can’t do it for $400. Can I get anywhere close so I can compete and still make an income where I’m happy and still meet my goals? So, starting 2005, I traveled all around the country trying to find other dentists who had been in similar situations and made it work. I traveled to Florida to visit Vincent Monticello, Baton Rouge to visit Dr. Bob Westinman, Scott Perkinson in Houston, Texas, Roy Smith in Tyler, Texas. I went to 19 places, and I would always visit with them. Some places would let you come but you had to pay a little fee. That’s fine. I didn’t care. I figured I would make it many times over, and I did.
So, I studied that, and I developed a plan where I figured if I could just completely eliminate all the real waste in the practice and systematize every process, then I should be able to steal enough of the time I was spending in a patient day and apply that to doing more dentistry. As long as I was wise enough to market wisely, change the perception of who I was in the community from a high end hoity toity guy to a blue collar guy that just wanted to help you and do work.
So, it was a several year process. We ended up doing that by 2008. I went to a five day week dentist producing about a $500,000 a year gross to a three day week dentist producing three times that, which is about three times the national average that they publish. So, you got to feel pretty good about that, and I felt like the quality was still there. We were doing a lot more dentistry, but I was three a week. You’re not that tired at the end of the day. You get home and everybody’s happy.
So, then, l taught that all around the country about how we did it, and the whole time I was teaching it there was something missing. I really didn’t know what it was until this past winter. So, let me tell you what happened. So, I’d gotten somewhat successful, published a book called “Time Genius”. The president if Mississippi State University actually came to my dental office and talked to me 15, 20 minutes one day and said, “You know, Chris, I think some of our students could really learn from your experience, your successes, your failures, how you went from engineering and all that.”
So, I agreed to go speak to an entrepreneurship class at Mississippi State this winter, and I get down there. It was a real bucket list. I mean can you imagine the president of your alma mater asking you to speak to an actual class where they’re getting credit. I mean that’s amazing. This is actually the room where I took Psychology 101. It held a few hundred people. I mean it was just a dream come true, but we’re down there. I’m talking to them and having a great time. The dean walks me back to my truck.
As we’re leaving the auditorium, the dean says, “Hey Chris. Obviously you studied lean manufacturing. It’s not surprising with your engineering background,” and I said, “Professor, they must not have gotten to that by the time I swapped courses on the engineering because I don’t know what lean manufacturing is.” He stopped and looked funny. He said, “Well, you just got up in front of those kids and described an exact model for making lean manufacturing work in a health care environment.” He said, “You ought to learn more about it because that’s what you’re doing even if you use some of the wrong terminology.”
I said, “Hey.” That’s my personality. I went home. I go to Amazon.com, order about 10 books, and read them cover to cover as soon as they come in. That just opened my eyes to a new world where I always had certain things that work, but I didn’t really understand how to put them together into a blueprint like Lorne talked about earlier, the high capacity blueprint.
When I read those books on lean management and the way that Henry Ford really began the concepts of lean management 100 years ago. After World War II, the greatest business minds in the world went over to Japan to build their economy using those principles, the Japanese took those principles and really took it to another level. They took it to another level. They created a culture based on lean manufacturing principles that had originally come from America.
When you read those books by the Japanese folks it is amazing the detail that they went into. As I read it I realized there is not really one contraction in the system of how they say and do things, let’s say building automobiles, and how we do it in our practice doing teeth. The Japanese, they always talk about continuous improvement. Their word for that is kaizen. I always say this when I’m doing my lecture, “If anybody out there is from Japan, raise your hand,” and if somebody raises their hand, which is rare, I say, “Look. I’m about to butcher your language. Please forgive me.” So, I’m about to mispronounce a bunch of names, but if you’re not Japanese, you’re probably not going to know the difference.
So, kaizen. That concept in of itself is a very simple concept, but that’s what we always try to do here in the dental practice. When we started doing our system a long time ago, I got to thinking it would be nice because there’s a furniture factory in town. Those concepts could turn out a lot of recliners. Maybe those concepts would work in dentistry, but I would always think, “Yeah, but when we’re building a recliner, we’re building 1000 at a time of the same thing.” It doesn’t work in dentistry. You’re doing fillings, root canals, whatever. The end product is far too customized. Even tooth fillings are like snowflakes. There are no two alike, and with root canals, it’s just impossible.
As I read those books I realized that that true end product in dentistry is not the filling. It’s not the crown. It’s not the root canal. The true end product is always chair time. That’s a pretty major concept you need to get into your head if you’re going to follow my sample. You’re not building crowns and fillings. You’re building chair time.
Now, the experience that the patient has in the chair may result in what type of dentistry they get. They get a filling. That’s customer experience. That’s not the end product. In our practice, we’re always conscious. We’re trying to produce as many set up rooms, ready for the patient with chair time as we can in a day, and that chair time, even though it’s an abstract concept, is our end product. That is our Ford Model T. That is our recliner. That is whatever our factor might be producing. Our product is that chair time. If you understand this as we go through this a lot of this will make better sense.
So, to start this out, let me just go through and let me just share some common terminology that they would use in Japan to their clients in the dental office. So, one of my favorites is poke-yoke. Now, this is a term that originally meant to “full proof” something. So, in Japan, they’re always trying to make sure that no matter what, the workers always have a system that never allows them to mess up without a bunch of safeguards coming down.
So, in a dental practice if you think about it, one of the things that whenever I interview a dentist in a seminar, ask their opinion about anything, no matter what, they’re always saying to me, “Hey, Chris. I have trouble with my assistants. I love my assistants. I love my team, but they have trouble. A lot of times, when I come into the room, they get up to go get something from the storage, to get a supply o to get something like that.”
Long ago, before I knew about lean management, we came up with what we call ten flex, and there’s a good example just on that website I gave you. These are in my office, they’re color coded to what I show you. In this particular procedure, orange is going to be a composite resin. So, these are laminated posters, and we lay these down on the counter behind the dental chair 12 o’clock to where the assistant works from.
Each block represents one item that I need to complete a composite resin. So, here, you see PDL syringe, loaded syringes, all this stuff. So, the concept is if the assistant lays the correct template down behind the chair, and they place each of the items on the block where it says composite gun, curing light, if they lay it right there. Each of these blocks fits, by the way, the item you’re laying on there. Then, after they’re through putting the supplies behind the patient, they look at this template. If every block is covered, then the procedure is ready to go. There’s no supply missing. That’s the whole concept of full proofing a room setup.
Here’s a good one, the concept of kanban. Now, in a furniture factory or a car plant, a kanban, the word actually means single card, but above everything else, there might be a giant illustrator. There might be a big TV screen, and it’s going to keep statistics on it. It’s going to let them know where they’re at, how their doing, how they’re proceeding throughout the day. There’s a Toyota plant 20 miles from Ripley, Mississippi now, and a lot of these concepts is right there for me to look at.
So, in our office, we try to figure out how we can put something somewhere in the office that keeps everyone on target and let’s everyone know how the day’s going, what needs to be done next so the doctor can look it at a glance and know where they need to go to next because, in my opinion, the doctor should never be rushed with the patient. The patient comes here to get treatment from us. No matter how much dentistry you’re doing, you owe it to that patient to be calm, collected, and focused on them when you’re seeing them.
I will not condone somebody that rushes through the day and tries to be fast for the sake of being fast. No way. You’ve got to be focused. You’ve got to do the patient right, and you’ve got to do good dentistry. This kanban board, we call ours the route board, allows us to do this on our practice, and this board is kept in a central location. It’s in our sterilization room now. It used to be in our hallway. Now it’s in our sterilization room now. We actually have a closer look at a TV feed that shoots it around the office all the time. So, I’m never more than two steps away from seeing everything that goes on in the office.
Obviously, you could do a whole day’s lecture on this thing. We can’t get into a lot of detail, but the whole concept is there is a board somewhere in the office that everyone can look at. Don’t tell me I’ve got software, I’ve got live systems because I’ve done it all. I’ve done it all in combination, but this board, broadcasted around the office, will beat any other hands down if it’s utilized properly. That’s just like anything around here. You have to utilize it properly.
3D Cat Scans in Dentistry P3
I was at an advance course in radiology and one of the servants there we were looking at a cat scan and he said “that’s an apical scar, that’s not pathology”. I don’t know what an apical scar is, do you guys know? That’s not healthy. Look at this, look at the cortical plate can you see that it’s perforated right here? Here’s an axial view. Look at the cortical plate on this size, it’s in tact. You absolutely cannot find these with digital x rays. Even with a 3D CAT scan if you guys had one within a month you would be able to do this. You can see things you just can’t see anywhere else. Look at the legions here and the ones here. Again you can see how we don’t have the full side view of the tooth, that’s because I’m moving in ND out. That’s because I want to know if the bone and the tooth fit together like this. If they don’t then there is an issue, there’s a problem here.
This is an every close friend of mine. I’m not her dentist, she sees somebody else. she actually came by the office one day and I said ” let me do a cat scan for you ” and she let me do that . She is very traditional maiden dentally and medically. She now has another root canal treated tooth. She now has been diagnosed with autoimmune disease and she’s 45 years old. I don’t know if she’s going to do anything about it. It doesn’t hurt she said. Look at this, this is that same patient. Look at the legion on the distal root. The immersion root has three canals. What I’ve seen is what I believe for a long time. I’m not sure in my mankind, in my opinion that this is physiologically even possible. I’ve got three canals and immersion root but guess what we still have a failure here. This is another root canal failure tooth. A woman came in about two months ago and right off the bat I was taking her health history and right off the bat she mentioned to me my daughter who was 4 months old died last year. I wasn’t trying to be a psychiatrist but I put my arm on her and said ” are you still carrying guilt about that ?” she looked at me and said ” I’m dealing with it I’m a psychiatrist.” I found out later she got the biochemistry award when she was n medical school. She’s a very bright girl. She went back and did an autopsy on her four month old child that’s dead, she came to the conclusion that her child died because of excessive vaccination. She’s really gotten on the bandwagon. Now she’s also interested in her own. When she started opening up that door and that window she found like we have found that there’s a whole world out there. when she started getting interested in vaccinations then she started getting interested in holistic health and she like a lot of us , I don’t know about you but I absolutely believe that the traditional medical model was the correct model 300 years ago and it took some failures to fund out that it’s not it.
Here she is right her. Can you see the radio ligancies around those from an apical view, same thing here? This is a patient I think I saw last week. 90% of the patients I can show you something interesting on the CAT scan. its real clear from the very beginning when you look at a cross sectional view it now lets you decide I’ve got some problems I’m going to take this tooth out, do I want to do a bridge , do I want to do an implant? Everybody will decide for themselves what they want to do about that but know you’ve got a piece of the puzzle unless you could do an implant if you wanted. In any way you know before you g o in what the issues are. How do I evaluate the CAT scan? Is there radio ligancies? How big is it? How does it compare to other teeth in the same scan? Can ii see it in other views? I like more than one source but sometimes you get one view that is so dramatic that it just nails it. How sick is the patient? How healthy of do you want to be? I don’t have a different criteria for root canal treated teeth. To me they should look as healthy on the CAT scan as a non-treated tooth. I see a lot of cancer patients in my practise and again I’ve seen one patient that hasn’t had a lot of denture. Amira’s belief, we’ve talked about I which is cancer is an infection that thrives in the presence of heavy metal. This patient I’m going to show you had breast cancer, I think she came in last month. Metastatic legions already to the sternum look at the first molar. I don’t think it’s over I don’t care if she has a metastatic legion to the sternum. I don’t think her life is over. Look at the legions here. Again you have to look for them but they’re there.
Everybody has to decide if this were you wife own you’re going to treat it. I had a patient about a year ago who didn’t really believe in what we do drug in by sister in law with brain cancer. I called the physicians and u Sid “we have some infections found in the CAT scan” and he said to me almost verbatim “let’s not bother, he only has four months to live.” There will be those people in there that will say that. Actually he would not let us treat. He really never bought into this and he didn’t last 6 months. How would you treat it? A milphonic patient this is that same patient, look at the legions there. This sis the patient that is would look at in depth. I’ve seen amazing results when the world cavity s treated as one of the problems there is no guarantee what would you do if it were you or your family member . Would you get rid of the infection? Would you try to improve the immune system? I don’t treat cancer. patients must be under the care of a health practitioner and that’s not for medical legal reasons that’s for me personally. Vie had one exception and then I’ll talk about it. It’s always the decision of the patient. I believe that most illness is an infection of immune break down including cancer. Why do almost all cancer patients I see have extensive dentistry, mercury infection, root canals? The best way to retreat it don’t wait till the boats down. What does that means to you? what that means to me is I don’t know about your practise but I’ve seen these cancer patients and they’re not coming in for me to treat their cancer , they’re coming in because they found out that there is a connection between oral health and cancer. Why wait until they’ve already got it. What if we would get ourselves and our patients to do all these stuff first. This is the kind of view that we’ll see from a cat scan.
This is a 50 year old patient she came in post or to, her <inaudible> teeth were a little mobile but I wasn’t sure if they were not. She wanted beautiful teeth and beautiful smile, she wanted a full moth reconstruction. I’m not going to go into how and why we would treat this all I ‘m saying sis the more you know to begin with the easier it’s going to make her life. In this case there was a bundle on the top of the nerve. Where is the third molar in this panoramic view? You really can’t see it but look at it over here you might see of somebody has got another. I’ve done at least 6 000 third molar extractions. I just think the chances of that ended up in the middle of the sinus could wreck my morning or afternoon. All it tells me is that beforehand keep me out of trouble. Eagle syndrome, it amuses me how many of it’s I see. 40% of the patients have <inaudible>. Ten days ago we were working goats. that means you got to look at all their eyelids, you go to trim all of their feet , you’ve got to put them in the head gate and some of them get turned around and when they get turned around you’ve got to pick them up and get them out. About four of them got away. They’re on the ground they’re bout a 110 pounds. I’m jumping on top of those with my son. I told him beforehand I said I’m just going to watch. It took me about ten days for me to be able to walk normally I would be afraid to fall jumping off that thing.
I’ll tell you my theory on this. I think one time they were osteoporotic or what happens is when the body becomes acidic the body pulls mineral from the bone if it doesn’t have enough ninny solution or available to buffer. When it pulls it out of the bone it gets in solution and then it gets deposited in different areas. Those will be your calculus formers and those will be your eagle syndrome. There’s nothing I can do about it but it’s kind of cool and fits into our holistic approach. My treatment is I use coral calcium plus aloe vera you can check their. There’s other things we can do but rode what I’m really trying to focus on is just this. All of us that are lecture can lecture on a lot of different things.
I got really involved in sleepabania or airway disturbances a long time ago and haven’t done that in a while. this is an area that is underdeveloped but it has the potential for you to look at the airway at this because if you hadn’t put their front teeth together and you get your cat scan and the airways open it can tell you a lot of things. Here’s a couple of our Clydesdale and lets change direction for a second. This is why most people buy CAT scan there is no question about it. You can do some amazing things with this with implants. You can instantly go in and look at the bone from a cross sectional view, an axial view, you can drop a virtual implant into that place see where it will fit. You can map the infernal v alert, you can look at the sinus, you can look at all of that in seconds or minute. You may want to take more time later but you can do that at any time. you can plant implants quickie you can decide to refer a knot , you can order surgical stamp , you can in the fire connect to a Sirac and what I’m waiting for is to be able to do a surgical stamp on the sire and then tell me that its really coming out really quickly and reduce impact in he tory . It’s not a guess work you’ll know if you place an implant what size, diameter you’re going to have. I’ve heard a young guy lecture twice, tells me that he schedules an implant patient fifteen minutes. I’ve actually seen him do it, that’s with a surgical stamp because there is no flap, put the surgical stamp in. I have placed about five zirconium implants in the last three or four months. First couple of times we orders those from Germany it was ugly. a lot of those things you think ids going to be simple , one of the things that we figured out that you can do is if just a bet registration inside, you get this guide that comes from Serena and you have to attach that to the teeth and then you put that in and you take a cat scan . This is one that we did with a zirconium implant and it really helped because it makes it so simple. You know exactly which angle it’s going to be so you can do some virtual planning. It’s going to evolve its going to get better.
This is one of or patients that came in, we’ve decided together that we were going to do an extraction on that tooth. She shows up in the office and sys by the way can you put an implant in today. It was not schedule today but look at it, who difficult is that? The nerve is way down here, plenty of room, not a lot of infection. I didn’t do that very often but it has some amazing ability. if you decide that implants weren’t for you philosophically I strongly recommend that you get a 3D cat scan , don’t do all of them just do the slam dunks . Do the easy ones, send the tough ones to your old surgeon out or somebody else. Lessons learned from a clinical rancher and I’m at heart a good simple herder and rancher but I love all of these stuff. We are at the start of new technology if this fit your hedgehog concept, get ahead of the curb. Don’t wait till you are the last person on the block to do it. What do the small legions mean? I sometimes feel like madam Currie. I haven’t seen anything like this since I’ve been in practise technologically. I’m seeing things that nobody knows what means. I’m ting to figure it out but this technology is fascinating. I think we need to be more aggressive about what we do. The CAT scan is a great tool for early detection it let us see low grade chronic infections of long standing. Most legions are symptomatic. Like the goat, catch it early, it helps in case and implant planning, wows the patient, it financial creates an amazing amount of dentistry.
What’s the difference between early detection and prevention? For me it’s still a moral issue. Early mental detection can be a systemic prevention. when I was overseas I walked into the first airborne camp , no hawks, no doves , all eagles . Most of you don’t know what that means. What this meant to the 110 first bronzes in this unit is don’t get distracted. We have a mission to accomplish and let’s just be eagles and I firmly believe that this organization stands for that. There is a lot of distractions that I see out there that I see this organization being the forefront, staying focus and taking care of these patients.
7 Smart Things You Can Do To Eliminate Bad Toenail Fungus
 You don’t have to live with toenail fungus. There are dozens of things you can do to treat your painful, yellowed or deformed toenails. They range from simple home treatments to highly effective medications to surgical intervention.
You don’t have to live with toenail fungus. There are dozens of things you can do to treat your painful, yellowed or deformed toenails. They range from simple home treatments to highly effective medications to surgical intervention.
Millions of people just like you live with toenail fungus when the don’t have to. If you can clear the fungus from the nail and from the nail bed, you can grow an entirely new, clean and beautiful toenail. While a new nail can take up to a year to grow, it will never happen if you don’t take action now.
How To Get Rid of Toenail Fungus:
There are safe and effective things you can do to get the process started, including the following seven very smart ideas
1. Take systemic antifungal medication pills. These include clotrimazole, itraconazole, terbinafine and others. They very literally cure the problem from the inside out.
2. Turn to topical antifungal medications that you paint on infected toenails or apply as an ointment or cream with a swab. In some cases, the topical medication can be combined with systemic medications for quicker, better results. Topical drugs include ciclopiroxolamine and ciclopirox, among others.
3. Consider laser treatments. Designed just for this purpose, there are many types of laser treatments than have proven effective, including Fox Diode laser therapy and Pinpointe-type therapy. They disrupt the infection by killing the fungi so healthy nails can grow.
4. Explore surgical debridement. That’s the technical name for the removal of the infected toenail or a portion of it. With the damaged part taken away, healing and regrowth is easier.
5. Opt for surgical nail matrix destruction. This is a last-ditch effort to completely destroy the toenail. With this kind of surgery, the nail never grows back but it eliminates the problem. This is only done when other treatments have failed and there’s nothing else left to try.
6. Try one of the many different oils that help kill nail fungus. This includes tea tree oil — a smelly but effective antimicrobial agent — as well as grapefruit seed oil and thyme oil. Pure orange oil is also believed to work to cure toenail fungus, but very little evidence is available.
7. Use home remedies. These include a homemade mixture of rubbing alcohol and vinegar that’s said to be especially effective as well as snakeroot leaf extract — and even Vicks VapoRub applied before putting on socks.
You also might get good results from increasing your overall health with vitamin and mineral supplements that can improve your immune system. Massaging to improve circulation helps too. And the list goes on. It’s also important to clip away as much of the bad nail as possible as soon as you can to prevent spreading of the fungus and to allow treatments to get to the nail bed.
Whatever you do, don’t sit idly by and let the problem persist, getting worse and worse with each passing day. There are good options available to treat toenail fungus.
For more information, visit: http://www.mommyedition.com/how-to-get-rid-of-bad-toenail-fungus
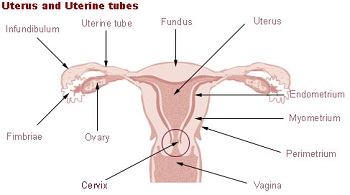
Can STD Cause Cervical Cancer?
Cervical cancer is one of the most common forms of cancer and is caused by the HPV virus. The human papillomavirus belonging to the papillomavirus family of viruses can be passed from one human to another through genital contact, vaginal or anal sex and in some cases through oral sex. Commonly the virus goes away without any severe health effects but in some cases it can lead to modification of normal cells into abnormal cancerous cells causing cervical cancer. It is most common in women and develops around the uterus and vagina. It can lie dormant for several years and can easily go undetected.
The Pap smear test is the most common test for detecting pre-symptomatic stages of cervical cancer and can help in early detection and prevention of cervical cancer. This test is cheap and can be done in many hospitals. Women are encouraged to take this test every 5 years and maintain healthy sexual contact throughout their lives. Negligence on the part of sexual partners can easily lead to one transferring the virus to other.
The HPV virus exists in about 100 different strains and two of them 6 and 11 produce very painful genital warts. About 70% of people come in contact with the HPV virus in their lifetime. Warts are clot like structures and can be a big nuisance. They are one of the symptoms of HPV that can be visibly diagnosed. Many other forms including the deadly strain 16 can go undetected in early stages and cause half of the cancer cases.
Though a deadly disease HPV is very different from HIV in terms of symptoms and effects. HPV virus unlike the HIV virus lives on the skin cells. The HPV virus can cause various health problems like genital warts, cervical cancer or Recurrent Respiratory Papillomatosis (RRP). As is always said prevention is better than cure. HPV vaccines should be given to children of the age of 11-12years. These vaccines are completely safe and effective. With our current generation getting proper knowledge of AIDS and STDs. Knowledge about the HPV virus is equally important amongst youngsters. People should take necessary precautions while having sex and limit their partners to avoid infection. Condoms cannot completely protect you against HPV as it is caused by physical contact of genitalia.
Yes STDs can cause Cervical Cancer and everyone especially women should undergo regular tests throughout their lifetime and lead a healthy sexual life to avoid this disease.
Do Anti-Aging Creams Really Work?
If you’ve ever tried an expensive anti-wrinkle cream, only to find it didn’t give you the results you hoped for, then you’re not alone. Millions of people try these products every day, only to find they they are no superior than their everyday moisturizers.
But does this mean all anti aging creams are a waste of money? Not at all. In fact, recent developments in skin care science mean there has never been a better time to find product that can legitimately reduce the sign of those fine lines and wrinkles. But the secret lies within the ingredients the product uses, and not the over-hyped marketing that many skin care companies take part in.
With this in mind, here are a few crucial ingredients to look out for (if you’re serious about finding something that works).
Retinol
This is the king of anti-aging skin care ingredients. It’s essentially a vitamin A compound that works to create new growth of collagen and elastin. Additionally, retinol is one of the few ingredients which has shown undeniable proof of efficacy in dozens of clinical studies. So if you want a powerful anti wrinkle cream, check the label to see if it contains this crucial ingredient.
Hyaluronic Acid
One of the most common reasons why fine lines and wrinkles develop is due to lack of hydration within the skin cells. Using a topical moisturizer is crucial, but it’s equally important to make sure your skin is hydrated from within. The first step is to make sure you’re drinking enough water each day, and the next step is to make sure your levels of hyaluronic acid are up to par. This ingredient can be absorbed through your skin, and it increases your natural ability to hold moisture inside the skin cell. This can give your skin a younger, plumper, firmer appearance – and it can also help to diminish the appearance of wrinkles.

Unfortunately, many people waste money on anti-wrinkle creams which don’t live up to the hype. But with a little research and insight, it’s possible to get excellent results with over-the-counter creams, just as long as you stick to products which use proven ingredients. In fact, the lifecell wrinkle cream formula contains both of these ingredients, so this is certainly a good option (but unfortunately, it isn’t cheap).
The tips in this article were provided by Rita Brooks, a natural health enthusiast who specializes in skin care advice. Be sure to check out her detailed reviews and natural health guides. You can find her blog at ritabrooks.com
How To Remove Cellulite Using Body Wraps
Cellulite is a problem that most females will experience at some point in their life. For years experts have been trying to identify the true cause of the development of cellulite, but no one knows for sure what actually causes these unsightly dimples to show up on the skin.
Some experts believe it isn’t just one thing that leads to the development of cellulite, but a variety of different factors. Some of the things that can lead to the development of cellulite include diet, lack of exercise, the clothes you wear, genetics, age, and bad habits like smoking.
Regardless of what causes it most women are on the look out for a proven way to get rid of cellulite and keep it from reappearing. There are various options available that can help reduce the appearance of the dimples and bumps caused by this problem. However, anti-cellulite wraps are among the most effective treatment method of them all.
Compared to cosmetic surgery, body wraps are a very cheap way to treat cellulite. These wraps help get rid of cellulite naturally because they have certain ingredients inside them that help draw out the fat toxins that lead to cellulite formation.
First you need to buy a good body wrap. You can find some really good ones on the Internet, but there are also some health food stores you can visit that will have them on sale too. All anti-cellulite wraps are not made the same, as they all contain different ingredients which serves a different purposes.
If you wish to keep your body protected from free radicals that cause cellulite then go with a vitamin E body wrap. If you want to draw out the toxins that are often responsible for cellulite showing up you should go with a clay body wrap. If you notice that your skin has been damaged by cellulite you should invest in an almond oil body wrap, as it will soften and moisturize your skin.
Fluid retention is also a common cause of cellulite, and a body wrap that contains juniper berry will help you reduce fluid retention. A lack of blood flow can also lead to the development of cellulite, which means you should definitely get a body wrap that contains either caffeine or rose oil in it because they both will help improve your blood flow to the problem areas.
Once you have the right body wrap all you will need to do is put it on the affected area on your skin and then your skin pores will start to open up. Once your pores open up the wrap will start to draw out the toxins and fats that are causing cellulite to develop right below the surface of your skin. Until the cellulite is finally removed the fatty tissues will break down gradually.
Even though body wraps are very effective you shouldn’t only depend on them. Follow a healthy diet that includes many green vegetables along with applying the wraps to the problem areas on your skin. Also, you will have to keep on applying the wraps consistently in order to notice your cellulite disappearing.
The fact that body wraps are inexpensive and effective makes them worth paying for. Most women also love using them because they are an all-natural method, they don’t cause any pain when you use them, and they are very easy to use. Probably the best benefit of all is the fact that they don’t cause any adverse effects like some other treatment methods do.
Lecture on Dental Materials P4
So anyone know what amalgam is? It isn’t that way to get that right. One of the components is and you can see why we don’t have so much of this technology any more, mercury. But there was a time when this was the dominant one and probably if you’ve got grandparents or great grandparents, you may even have a scenario where they had silver or gold as their filling, right? So not very cost effective, but it made for a good filling, mostly because it was malleable and inert. So it’s liquid at room temperature, reacts with silver and tin and essentially forms a plastic mass [at times]. So in essence it was the precursor to the bone cement concept, right? You could have something that was workable, shapeable like a dough and then you could plug it in and it would set. So in a matter of moments, you actually had a hard material that was capable of supporting load.
Nickel titanium, which also we call nitinol. So that’s a 50:50 alloy. Gold, again not so common anymore. Probably the acrylic resins at this point dominate. So those are based on polymethyl methacrylate type resin chemistry, very much like bone cement, sets up very, very quickly. Dental works a little bit different from the orthopedics and not — Dr. Reese made a comment about bone cement, I think I made a comment about the bone cements, Dr. Andy Combs made a comment about bone cement, it’s a two-part system, you’ve got pre-polymerized powder and then bring it in except that it’s a chemical hazard to get the monomer in here. You’ve got a monomer that starts that process, you’ve got a liquid vial and then you’ve got a little packet of pre-polymerized powder, put the two together in a bowl, mix it up and you essentially start to dough a mass. So it starts as something that’s almost fully liquid like pancake batter and then ends up something like plateau. And so in a matter of 3 to 5 minutes you move from a liquid to something that feels like plateau. And as it goes through its polymerization process you’ve got a very high temperature increase, so up to 100 degrees or 150 or so degrees Fahrenheit. So it gets so hot you can’t even hold it in your hand any more. So that part of the experiment is great to show the class, it’s the monomer part. So I used to bring it and do in class and I think truly it’s an environmental hazard. So we won’t do that.
Just take my word on it but that same concept really was important but have any of you had filling work in the last few years of any sort? Did you experience that technology? Probably not. So more likely what they did is that they took the same resin chemistry, but they used a UV curable polymer. So more likely they just set something up in your mouth and then a lot of times, they just do UV exposure and this thing sets up in a matter of moments. But they also have quick setting, but yeah, most of us, right, we have our jaws probe tube and probably aren’t seeing anything. But the chemistry is very, very similar to what we’ve seen in orthopedics and the scent is very similar. So if you recall that odor, you can imagine working in the OR, where you’re going to have 12 to 15 packets of bone cement go by. So environmental issues are an issue which probably explains some of the spacesuit technology. You were in surgery recently? Yeah. So they were in full mask, not just for blood contamination, but there’s a lot of — anytime there’s bone cement you have to look at the outgassing of that monomer. So it’s a real environmental concern. It’s really bad. Yeah, you probably weren’t suited up with that protective gear, yeah.
So if you go and watch a surgery, just be prepared for the other side of that. Actually if any of the nurses are expected, I believe they have to leave the room, it’s that bad. Yeah, so it’s a – there are some downsides of medical technology.
Okay. Thermal expansion coefficients, so like I said, it’s the only place in the class where there is an opportunity to talk about thermal stresses because we really don’t have to deal with that anywhere else. Just a simple analysis, here’s our thermal expansion coefficient alpha, which is the length change delta L, normalized by the initial length for a given temperature. So what that means it is we’re looking at a structure for simplicity sake, which is L0, we subject it to a delta T and then moving through that delta T, we get a coefficient of thermal expansion. So there are only a few scenarios where we have materials that give us a negative thermal expansion. So for the most part we apply delta T, that temperature increase, we move from L to a deformed or expanded length L and so it’s alpha is our change now. So this essentially is this differential here, so it’s the total length change delta L normalized by the initial length L0, multiply that by delta T. And the strain that we get as a result of that – and again we’re assuming isotropy. So isotropy is assumed, the way to get around that would be to do this directionally, right? So just take different orientations and then you could get thermal expansion efficient in a longitudinal axial or circumferential direction.
So the strain is just that thermal expansion coefficient times the delta T. And we look at the biometric thermal expansion coefficient we’ve got the biometric strain, which is three times alpha. So again just alpha coming back to give us deltal L over L0 times delta T. So just a very simple expression.
And I gave you on this worksheet that you downloaded, what happens as a result of thermal expansion coefficient? So it’s a really simple problem. It’s not to show dissimilar the schematic that we have here. Not so dissimilar from what we had when we talked about transferring stresses or looking at composite type behavior. So we’ve got an internal structure, which is in gray. That’s our filling and we’ve essentially reamed out a hole in the tooth structure. So we’re going to assume that we reamed out a nice cylindrical hole. So again you’d have to account for what the geometry is of the hole itself and so we considered here a 2 mm diameter hole, which is 4 mm in length in a molar tooth. So we’ve got a hole that we’ve created, that’s got 2 mm diameter and it’s sitting in a tooth structure. So here is our tooth but we’re just going to schematically say well, it’s got a boundary and we’re going to be [interested]. So we’ve got a diameter of 2 mm and we’ve got a length of that hole which is 4 mm.
And then we look at what’s going to happen to the coefficient of thermal expansion? So in other words, what’s going to happen if we think about this rigid boundary of the tooth acting on this material? So we’ve got a void space and then we’re going to fill that void space with a material. And then we’re going to subject it to a temperature fluctuation, delta T. And then the question is what’s going to happen to that structure? Well, there’s going to be a thermal expansion of that material as it’s heated and then we have to look at thermal expansion mismatch between the enamel itself and the amalgam or resin. So we’re going to just treat this as enamel, and this is going to be our amalgam or resin. And we just look at the difference between the two.
So this basic problem looks at what happens with the delta T at 53 degree C? So we’ve got a delta T of 50 degree C and then we’ve got different thermal expansion coefficients. So we’ve got the thermal expansion coefficient of the amalgam, so there is our mercury alloy of 25 times 10 to the minus 6, again this is millimeters per millimeter. So it’s a length change per original length per degree C. So it’s unit less per degree C or strain units per degree C or strain units per degree C, alpha of enamel. So again a very small thermal expansion coefficient, which probably makes a lot of sense if we think about what thermal expansion coefficient means. So enamel will be a highly ceramic structure. So we’ve got very little exchange of strain as a function of temperature, so only 8.3. And then you look at the polymer, so again we think back to what polymers were, they were these open structured chain materials that are isotropic for the most part, but they’re also randomly organized in space. So there is lot of room for expansion.
And so even though these are somewhat rigid polymers, you’ve got a coefficient of thermal expansion here for a typical acrylic resin on the order of 81 times 10 to the minus 6. So 81 versus 25 versus 8.3. And then you look at – okay, well what’s the elastic modulus of these materials? So the elastic modulus of that alloy, so again steel versus a polymer, the amalgam is 20 gigapascals for elastic modulus. The resin is two and a half gigapascals, so again a much smaller elastic modulus, it’s a polymer. And then we go back to our expression for what’s the change in volume. So again the volumetric strain took the form of three alpha times delta T, right?
So the volumetric strain took a form of three, so we look at delta V, so that was our volumetric strain, when we look at delta V we’ve got whatever the initial volume is and then we’re multiplying that times – three times alpha times delta T. So we’ve got change in volume is the initial volume times three times thermal expansion coefficient and it’s assuming isotropy times delta T. And then you plug this in, and say, well, what’s going to be the change in volume if we use the mercury-based amalgam? So again just geometry, what’s the cross-sectional areas? We’ve got pi times the radius squared. So pi times one millimeter squared times the length, so we’ve got 4 mm of length, then we’ve got three times that difference now in thermal expansion coefficient. So we’ve got 25, which came from the amalgam, and then we subtract away 8.3, so we subtract away the thermal expansion from the enamel, that was to — 10 to the minus 6 power times the temperature flux 50 degree C. And so you get a volume change of 0.03 mm cube.
If you do the same thing for the resin, so again the same geometry would be pi times one millimeter squared, piR squared times the length 4 mm times three, and then the difference would be instead of having 25 minus 8.3, I’d have 81 minus 8.3, same temperature. And so now the volume change is 0.14 mm cube, so relatively large volume change. If I look at just a one-dimensional force span, you’ve got the forces of the elastic modulus times the strain times the area. So you’ve got the elastic modulus times delta T so that 50 degree C times the change that we have on the amalgam resin minus the enamel. So the difference between thermal expansion coefficient, whether it’s the amalgam or whether it’s the resin and subtract away from that the enamel and then you’ve got the perimeter of your pi DH, there’s your diameter, the height. And so you roll that out and you look at the forces and the amalgam force is 420 Newtons, the force in the resin is 228 Newtons. So the forces are relatively high.
But an interesting thing that I put here in gold is that although the resin expands, so if we look at just the delta V, you’ve got a fourfold increase in volumetric expansion. But the reduced stiffness actually results in a lower force. So again it goes back to — you can’t just look at – just when you look at back of the pockets or back of the envelope calculations, if all you had done (inaudible) to volumetric change, you would’ve said okay, just because of that thermal expansion coefficient of the polymer, the polymer does not look like the way to go because you’ve got a very high thermal expansion coefficient, if I run that into biometric changes you’ve got three times alpha, so there’s your roll right here, we’d have a fourfold increase in that volumetric expansion.
But if I convert that back to a force on the actual system because the modulus is so much stiffer for the polymer versus the metal, you end up equalized in terms of the actual forces. So your gut might have been to say, oh, four times the strain, I am going to expect to see a much greater contribution on stress or force. So just little plays on how some of these relationships work. So polymers because they have a lot of modulus make them very forgiving materials in lot of these applications. Question?
Question: Can you explain why you subtracted the alpha of enamel?
Lisa Pruitt: Because you’re looking at the differential of thermal expansion. So you’re looking at what’s the overall change. So you’re assuming at the boundary, the thermal expansion difference between how much – in other words, the thermal expansion is going to occur in the resin but it’s going to also have a temperature effect that’s going to be balanced by what’s going on in the enamel itself. So if you add delta T, you don’t just have the resin expanding, you also have contribution of what your dental tissue is doing as well. So you subtract that away. The same question, okay. Yeah, so we subtract out the counterpart, so we subtract that away because it’s also experiencing a thermal expansion effect.
So again that was very simplistic approach, just taking a simplistic strain, looking at how we can convert that to a simple force but it gives you perspective of just something we would design for differently in dental applications that we would never see in any of the other materials. So delta T issues are an issue.
So if we look at just some of the environmental effects, chewing forces, I think when you first think about dental applications, you don’t tend to think of the forces in the mouth being very high. And the forces in the jaw are extraordinarily high and if you look at [the bright] enamels, you can get extraordinarily high because it relies on their mechanism for prey and predatory effects. But just for a human a chewing force can be up to 900 Newtons. And so you’ve got a high cyclic loading capability. You can have large temperature differences. So we talked about 37 C being the sub-point and here in the mouth you’re looking at potentially a 50 degree C range. So you can run that through and not just singularly in one day but multiple times a day. So you just think about that effect of having something very, very cold, or something very, very hot and probably every one of you has done that, right, at some point, you’ve had something very cold and very hot or vice versa and you probably get a little tinge of nerve response when you did so. So there’s truly a thermal expansion that occurs and you can actually feel that right down to the innervated part of the tissue.
Large pH differences, so again enormous bodies of literature on the role of pH and the role of different types of a composition of saliva in various foods and how that plays a role of pH in the mouth. And it sounds silly, but it makes an enormous difference, large variety of chemical compositions from food, so I am sipping on my — we all have — some of us have coffee, some of us are chewing gum, we’re all loading our teeth in one way or another. So lots of issues.
Going back to what I started with, you’ve got a number of parameters to think about, you’ve got cyclic loads. So we have to think about fatigue resistance, when designing for these TMJ designs there’s a number of issues. There is overall fracture. So you’ve got a post-scenario, so you wouldn’t want to have fracture of the device. You’ve got again a bearing combination. So you’ve got metal on polymer, so we need to be thinking about wear assistance. You’ve got metal that’s now going to live in the presence of saliva, low pH, so you’ve got moisture, temperature and pH issues. So, you’ve got a big-time corrosion problems. And if we thought we had a corrosion design issue when we got to the Morse taper, you stick something in the mouth and talk about having crevice corrosion issues, you’ve got some design standards to worry about.